To fully evaluate a child with a suspected cardiac condition, one needs to go through the regular steps applicable in medicine. These are outlined below:
20.1 History
The history is traditionally divided into:
20.1.1 Prenatal
Prenatally, the history should delve into but not be limited to the following:
Infections: Some infections are the well-known TORCHES. They include Toxoplasmosis, HIV, syphilis, parvovirus B19 (fifth disease), varicella (chickenpox) and (Zika), Rubella, Cytomegalovirus, and Herpes simplex virus. Rubella, when acquired in the first trimester of pregnancy, is very well known to be associated with PDAs.
Medications: The use of some medications, including herbs, predisposes to heart disease in newborns. Anticonvulsant such as phenytoin, carbamazepine, and valproic acid are highly teratogenic.(Kalisch-Smith, Ved, and Sparrow 2019)
Recreational drugs: Excessive smoking, cocaine, and alcohol use in early pregnancy are all associated with teratogenic effects on the heart.
Maternal illnesses: Maternal medical conditions during pregnancy may be associated with heart diseases in their fetuses. Diabetes mellitus is particularly well known, predisposing to hypertrophic cardiomyopathy, d-Transposition of the Great Arteries, etc. Autoimmune conditions such as Systemic Lupus Erythematosus may also predispose to rhythm disturbances in the fetus and child, even when the mother is not symptomatic.
Family history of CHD: The recurrence of CHD in first-degree relatives varies but is almost always higher than in the rest of the population. For instance, having a first-degree relation with a cornoventricular defect is associated with a recurrence risk ratio of 24.3 (95% CI,12.2 to 48.7), 7.1 (95% CI, 4.5 to 11.1) for isolated Atrial Septal Defect, and 3.4 (95% CI, 2.2 to 5.3) for isolated Ventricular Septal Defect.(Øyen et al. 2009)
20.1.2 Perinatal
Perinatal history associated with heart disease may include the following:
Birth weight: A high birth weight, often associated with a child of a diabetic mother, is also associated with an increased incidence of CHDs. Conversely, a low birth weight may also be associated with fetal alcohol syndrome or congenital rubella syndrome, both of which are associated with CHDs.
Newborn resuscitation: Some critical CHDs can be similar to neonatal asphyxia in a newborn, thus requiring resuscitation.
20.1.3 After birth
Ascertaining history after birth is the most extensive. Many of these are directed to the features of heart failure. These include:
Growth failure: Poor weight gain is a very prominent feature of CHDs in children. Many clinically significant CHDs result in poor feeding, chronic metabolic demand on the patient and poor oxygenation in cyanotic CHDs. All these result in increased caloric demand, resulting in poor growth.
Cyanotic spells: Some cyanotic CHDs are associated with recurrent periods where the child has increasing cyanosis, sometimes associated with weakness, fast breathing and even unconsciousness. The presence of these spells may be a pointer to a CHD.
Squatting and exercise intolerance: Exercise intolerance is a common presentation of heart disease in children. However, for some cyanotic congenital heart diseases, most notably Tetralogy of Fallot, the added feature is frequent squatting when the child becomes fatigued.
Delayed milestones: Growth failure, easy fatiguability, and other genetic syndromes may delay motor milestones in children.
Others: Fast and sometimes difficult breathing are also common presentations of CHDs. Some children develop oedema.(Figure 20.1) This is predominantly seen in younger children’s faces and older children’s feet. Frequent lower respiratory infection is also seen in children with heart diseases, especially those associated with heart failure.
Uncommon symptoms: Uncommon presentation of heart disease in children include:
Chest pain is a rather feared symptom in adults but usually portends another diagnosis rather than heart disease in children.
Syncope can be observed in children with an arrhythmia or left or right ventricular obstruction. However, this is still not a common presentation in pediatric heart diseases.
Older children report palpitations.
Joint swelling does occur in Rheumatic Heart Disease, but again, it is not a common presentation in children with heart pathology.
Figure 20.1: Pedal oedema in a child with heart failure
20.2 Clinical examination
20.2.1 General
Clinical examination for a child with a suspected heart disease should always start as general. One should first look out for life-threatening signs and intervene quickly. Subsequent steps could include:
Nutritional status is vital as many children with chronic heart conditions with significant heart failure present with malnutrition. The growth pattern of the patient should always be evaluated.
Dysmorphism is very critical in pediatric heart diseases. As much as 23% of all children with CHD will have a chromosomal abnormality.(Wang et al. 2023) There are many genetic syndromes with well-documented recognisable heart defects. Below are just a few adapted from Ko (2015):
Table 20.1: Common genetic syndromes associated with congenital heart diseases
Coarctation of the Aorta, Atrial Septal Defect, Aortic Stenosis, Mitral Stenosis, Hypoplastic left heart syndrome
Alagille syndrome
90
Peripheral Pulmonary Stenosis, Pulmonary Stenosis, Tetralogy of Fallot
Colour: The skin colour of a child with a CHD could hold signs of its presence. Cyanosis, the blueish duskiness of the skin and mucous membranes can be seen in children with cyanotic congenital heart disease. This may not be easy on black skin and can only be observed in the mouth and tongue (Figure 20.2). Mild cyanosis is often not visible and may require pulse oximetry. Pallor can be observed in patients with heart diseases, such as Infective Endocarditis. Jaundice can be observed in patients with Infective Endocarditis or those with hepatic injury secondary to chronic heart failure.
Figure 20.2: Cyanosis in the tongue of a child
Clubbing: All four stages of digital clubbing are seen in children with cyanotic CHD or Infective Endocarditis. (Figure 20.3) Note that some cases of finger clubbing may be familial.
Figure 20.3: Finger clubbing
Respiratory signs: Respiratory signs commonly associated with heart diseases in children are tachypnoea, dyspnoea, chest recessions, and increased work of breathing. These are especially true when there is associated heart failure, which worsens with exercise or breastfeeding infants.
Circulation: The circulation in a child with a suspected heart disease is critical. Reduced circulation can be assessed with the warmth of the extremities, capillary refill time, and blood pressure.
Blood pressure: Low blood pressure is a late sign of circulatory failure and cardiogenic shock. Conversely, weak pulse may be associated with hypertensive heart disease as well. Wide pulse pressure, an abnormally wide difference between the systolic and diastolic blood pressures, may indicate a patent ductus arteriosus, aortic insufficiency or an aorticopulmonary window. Blood pressure should be checked in the upper and lower limbs as a higher BP in the upper limbs compared to the lower may indicate the presence of a Coarctation of the Aorta.
Pulses: The radial pulse is the most routinely examined in cardiovascular examination. It should be checked for the rate, rhythm, volume and character. If they are difficult to examine, especially in young infants, the brachial pulsus can be used. Other pulses should be examined, including the brachial femoral and dorsalis pedis. Next, the synchronisation of the radio-femoral pulse should be determined for a delay. This happens in the coarctation of the aorta. Pulses that are challenging to palpate or inconsistent could be caused by large artery arteritis, such as Taksyasu’s arteritis.
20.2.2 Precordial
Inspection: Inspection of the precordium yields a wealth of information in a child with a suspected heart disease. A midline bulge or left-sided bulge will often indicate a right or left-sided heart chamber dilatation. Visible precordial pulsation should be noted. Scars, especially from previous surgeries, are useful. Scarification, the usually small “medicinal” scars done on the chest as a means of treatment, should also be noted. A Harrison sulcus, depression of the lower part of the chest, is common in children with chronic heart failure and, thus, dyspnoea. Figure 20.4
Figure 20.4: Chest bulge and Harrison’s sulcus in child
Palpation: Palpation should be directed toward determining the presence of a thrill (a palpable murmur) heave at the apex or middle of the precordium. Also, a palpable heart sound, especially the second at the upper left sternal edge, may indicate pulmonary hypertension.
Percussion: This is of very little relevance in examining the heart in children.
Auscultation: Auscultation of the heart can yield a wealth of information. It should be done in a quiet environment, with the child as calm as possible. Auscultating can be performed with both bell and diaphragm. All four auscultatory areas need to be auscultated. Auscultating the back (between the scapulae) and over the carotids is always prudent. First, the regular two heart sounds should be determined. If muffled, they could indicate a pericardial effusion or sometimes obesity. Pulmonary hypertension and an Atrial Septal Defect, for instance could result in a loud or split-second heart sound. The presence of a third heart sound (S3) is not always pathologic in children, but an S4 is. The presence of a murmur needs to be determined. If present, it should be determined if it is systolic or diastolic and the point of maximal intensity. It needs to be graded (Table 20.2), and the presence of radiation must be ascertained. Table 20.3 indicates types of murmurs, their location and likely heart diseases. Diastolic murmurs are difficult to appreciate for the average medical student but may be present in aortic regurgitation, pulmonary regurgitation, and at the cardiac apex in cases of heart failure secondary to a large left-to-right shunt. Notably, approximately 80% of murmurs in children can be categorised as “innocent murmurs” as they are not associated with cardiac pathology.
Other sounds need to be evaluated as well. These may include a pericardial rub, which occurs in pericarditis, an ejection click heart in early systole and cases of aortic or pulmonary stenosis.
Warning: package 'tibble' was built under R version 4.5.1
Warning: package 'purrr' was built under R version 4.5.1
Table 20.2: Grades of murmurs
Grade
Description
Grade I
Barely perceptible
Grade II
Soft, but easily audible
Grade III
Moderately loud but has not thrill
Grade IV
Loud and associated with a thrill
Grade V
Audible with stethoscope partially of the chest
Grade VI
Audible with stethoscope off the chest
Table 20.3: Heart diseases and their murmur characteristics
Murmur
Location
Condition
Pansystolic
LLSB
VSD, Tricuspid regurgitation
Pansystolic
Apex
Rheumatic Heart Disease, Mitral valve prolapse
Ejection systolic
URSB
Aortic stenosis
Ejection systolic
ULSB
ASD, Pulmonary stenosis, Tetralogy of Fallot, Coarctation of the aorta
Continuous
2nd left ICS
Patent Dutus Arteriosus
20.3 Investigation
Various investigations used in the diagnosis and management of heart diseases are:
Pulse Oximetry: Pulse oximetry helps determine heart rate and oxygen saturation. An oxygen saturation lower than expected (<95% outside the early neonatal period) is considered abnormal and a strong indication of cyanotic heart disease in the presence of a non-pathologic lung.
Electrocardiogram: The electrocardiogram is a common modality for the bedside investigation of heart diseases in all age groups. It indicates the heart rate, rhythm, chamber dilatation, wall thickness, laterality of the chambers, electrolyte abnormalities and even the presence of a head injury. It is often not conclusive in many heart conditions but serves as a good auxiliary test in children, especially post-surgery. There are various types: The routine ECG takes just a few minutes to perform on a resting patient, usually lying supine. On the other hand, the stress ECG is traditionally done with the heart under stress, as may happen during an aerobic exercise. The Holter ECG, on the other hand, is attached to the patient and continuously monitors the heart for 24 to 48 hours. This usually gives a better reflection of the heart’s electrical activity over a prolonged period instead of just a brief period.
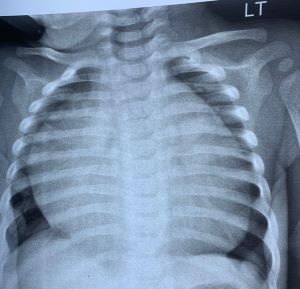
X-ray: A chest x-ray is very useful in diagnosing and managing heart diseases in children. Fortunately, it is readily available in many parts of Ghana. Both posteroanterior and lateral chest X-rays can be useful in assessing the individual chamber and overall heart sizes. Cardiomegaly, assessed with a cardiothoracic ratio > 60% in children, is seen in many cases of heart disease. Chest X-rays also indicate ling pathologies, often showing as opacification or silhouetting. Increased lung markings, for instance, can be found in patients with VSD and ASD, while decreased lung markings are often seen in the Tetralogy of Fallot and pulmonary stenosis. The shape of the heart is often an indicator of the underlying cardiac pathology. A Boot-shaped heart may indicate a Tetraloy of Fallot (Figure 20.7), while a globular-shaped heart points to dilated cardiomyopathy or pericardial effusion. Figure 20.6
Figure 20.5: Chest x-ray showing cardiomegaly and lung shadowing
Figure 20.6: Chest x-ray showing a globular heart
Figure 20.7: Boot-shaped heart of Chest X-X-ray
Echocardiogram: This is a rather old but new investigatory modality. It is old because it has been around since the 1960s and new because it is relatively new in Ghana. It is, however, a beneficial modality of investigation. An echocardiogram is essentially an ultrasound of the heart and great vessels. Its most significant advantage is its ability to visualise the heart in real-time, assess systolic and diastolic functions, measure chamber sizes and wall thickness, detect defects such as ventricular septal defect, determine valvular abnormalities such as stenosis and regurgitation, and even assess all these under stressful situation (stress echocardiogram). The video below illustrates the various echocardiographic views used in children. Unfortunately, since it is very user-dependent, it is not commonly available in Ghana, with pediatric echocardiography only currently available in Accra, Kumasi, Cape Coast and Tamale.
Computerised tomography (CT) scan and Magnetic resonance Imaging (MRI): These are more advanced modalities available for use, especially when an echocardiogram is inconclusive or further study of the patient is necessary. A CT scan generates the image using a series of X-rays taken at different angles without the complication of significant X-ray radiation exposure. Both modalities can employ contrast to delineate vessels.
Others: Other specialised investigatory modalities are used as required, including cardiac catheterisation in a specialised catheter laboratory.
Kalisch-Smith, Jacinta Isabelle, Nikita Ved, and Duncan Burnaby Sparrow. 2019. “Environmental Risk Factors for Congenital Heart Disease.”Cold Spring Harbor Perspectives in Biology 12 (3): a037234. https://doi.org/10.1101/cshperspect.a037234.
Øyen, Nina, Gry Poulsen, Heather A. Boyd, Jan Wohlfahrt, Peter K. A. Jensen, and Mads Melbye. 2009. “Recurrence of Congenital Heart Defects in Families.”Circulation 120 (4): 295–301. https://doi.org/10.1161/circulationaha.109.857987.
Wang, Huaming, Xi Lin, Guorong Lyu, Shaozheng He, Bingtian Dong, and Yiru Yang. 2023. “Chromosomal Abnormalities in Fetuses with Congenital Heart Disease: A Meta-Analysis.”Archives of Gynecology and Obstetrics 308 (3): 797–811. https://doi.org/10.1007/s00404-023-06910-3.